ECG changes in Hyperkalemia
There is no definite correlation between any ECG changes and the serum potassium - the relationship depends on individual patient sensitivity and the rapidity of development of the hyperkalemia
(* ECG signs may be absent if the onset of hyperkalemia is slow - as seen in chronic renal failure - even though the serum potassium is in the range of 7 - 7.5meq/L; by contrast, acute hyperkalemia can produce ECG signs at much lower serum potassium levels)
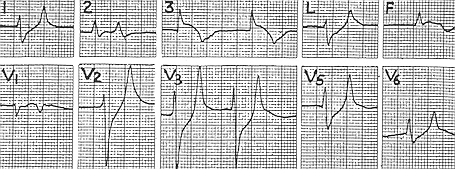
ECG showing tall T waves - "Tenting"
 Note the tall symmetrical T waves in the antero-septal leads
Note the tall symmetrical T waves in the antero-septal leads
ECG showing "thorn-like" T waves

ECG showing a "sine" wave pattern
 Note the wide slurred QRS complex which blends sinuously with the tall T wave into a "sine" wave pattern
Note the wide slurred QRS complex which blends sinuously with the tall T wave into a "sine" wave pattern
ECG changes "mimicing" an AMI
 Note the elevated ST segments in two of the inferior leads (S3 and AVF) suggestive of an inferior wall AMI, and the reciprocal ST depression in leads S1, AVL and V 2 - 5 Clues that suggest hyperkalemia = absence of P waves and the tall tented T waves in the chest leads
Note the elevated ST segments in two of the inferior leads (S3 and AVF) suggestive of an inferior wall AMI, and the reciprocal ST depression in leads S1, AVL and V 2 - 5 Clues that suggest hyperkalemia = absence of P waves and the tall tented T waves in the chest leads
ECG showing a "dumping" pattern
 Note the depression of the ST segments in leads V 2 - 6 - as if something "heavy" had been "dumped" onto the ST segment causing it to sink down
Note the depression of the ST segments in leads V 2 - 6 - as if something "heavy" had been "dumped" onto the ST segment causing it to sink down
ECG showing "Z-fold pattern"

Note the widening/slurring of the QRS complex and how the ST segment slopes straight up to the tall T wave producing a "Z" pattern
(* ECG signs may be absent if the onset of hyperkalemia is slow - as seen in chronic renal failure - even though the serum potassium is in the range of 7 - 7.5meq/L; by contrast, acute hyperkalemia can produce ECG signs at much lower serum potassium levels)
ECG showing tall T waves - "Tenting"
 Note the tall symmetrical T waves in the antero-septal leads
Note the tall symmetrical T waves in the antero-septal leadsECG showing "thorn-like" T waves

ECG showing a "sine" wave pattern
 Note the wide slurred QRS complex which blends sinuously with the tall T wave into a "sine" wave pattern
Note the wide slurred QRS complex which blends sinuously with the tall T wave into a "sine" wave patternECG changes "mimicing" an AMI
 Note the elevated ST segments in two of the inferior leads (S3 and AVF) suggestive of an inferior wall AMI, and the reciprocal ST depression in leads S1, AVL and V 2 - 5 Clues that suggest hyperkalemia = absence of P waves and the tall tented T waves in the chest leads
Note the elevated ST segments in two of the inferior leads (S3 and AVF) suggestive of an inferior wall AMI, and the reciprocal ST depression in leads S1, AVL and V 2 - 5 Clues that suggest hyperkalemia = absence of P waves and the tall tented T waves in the chest leadsECG showing a "dumping" pattern
 Note the depression of the ST segments in leads V 2 - 6 - as if something "heavy" had been "dumped" onto the ST segment causing it to sink down
Note the depression of the ST segments in leads V 2 - 6 - as if something "heavy" had been "dumped" onto the ST segment causing it to sink downECG showing "Z-fold pattern"

Note the widening/slurring of the QRS complex and how the ST segment slopes straight up to the tall T wave producing a "Z" pattern
Labels: CARDIOLOGY, Emergency Medicine, METABOLISM


<< Home