laparoscopic right adrenalectomy for pheochromocytoma
Labels: ENDOCRINE, GENERAL SURGERY
all you need to enjoy medicine. Daily medical Videos,Cases,Diagrams, Animation,Articles,Free medical books and news.
Labels: FUNNY MEDICINE, GYNACOLOGY AND OBESTATRIC, MEDICAL EQUIPMENTS
 Algorithm for establishing a diagnosis in chronic unilateral leg oedema
Algorithm for establishing a diagnosis in chronic unilateral leg oedema Labels: ALGORITHMS
 Note the tall symmetrical T waves in the antero-septal leads
Note the tall symmetrical T waves in the antero-septal leads
 Note the wide slurred QRS complex which blends sinuously with the tall T wave into a "sine" wave pattern
Note the wide slurred QRS complex which blends sinuously with the tall T wave into a "sine" wave pattern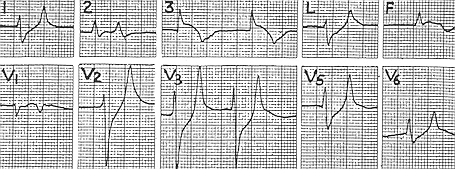 Note the elevated ST segments in two of the inferior leads (S3 and AVF) suggestive of an inferior wall AMI, and the reciprocal ST depression in leads S1, AVL and V 2 - 5 Clues that suggest hyperkalemia = absence of P waves and the tall tented T waves in the chest leads
Note the elevated ST segments in two of the inferior leads (S3 and AVF) suggestive of an inferior wall AMI, and the reciprocal ST depression in leads S1, AVL and V 2 - 5 Clues that suggest hyperkalemia = absence of P waves and the tall tented T waves in the chest leads Note the depression of the ST segments in leads V 2 - 6 - as if something "heavy" had been "dumped" onto the ST segment causing it to sink down
Note the depression of the ST segments in leads V 2 - 6 - as if something "heavy" had been "dumped" onto the ST segment causing it to sink down
Labels: CARDIOLOGY, Emergency Medicine, METABOLISM

Subscribe to
Posts [Atom]
