all you need to enjoy medicine. Daily medical Videos,Cases,Diagrams,
Animation,Articles,Free medical books and news.
Sunday, December 26, 2010
Nutcracker phenomenon
It results most commonly from the compression of the left renal vein between the abdominal aorta (AA) and superior mesenteric artery (SMA), although other variants exist. The name derives from the fact that, in the sagittal view, the SMA and AA (with some imagination) appear to be a nutcracker crushing a nut (the renal vein).
There is a wide spectrum of clinical presentations and diagnostic criteria are not well defined resulting in frequently delayed or incorrect diagnosis. This condition is not to be confused with superior mesenteric artery syndrome, which is the compression of the third portion of the duodenum by the SMA and the AA.
This Computed tomography for a 52-year-old woman with mild episodic gross hematuria revealed compression of the left renal vein between the superior mesenteric artery (SMA) and the aorta (Ao) before the vein merges into the inferior vena cava (IVC). This compression caused marked dilatation of the distal part of the renal vein (RV). The renal venous congestion caused hematuria, presumably through the rupture of submucosal veins into the renal pelvis. No treatment was given. Entrapment of the renal vein is a known cause of hematuria.
"Manual of Nephrology: Diagnosis and Therapy" by Robert W. Schrier
L W W | 336 pages | English | 2008, 7 edition | ISBN: 0781796199 | CHM | 2,0 MB
Now in its Seventh Edition, this best-selling Spiral Manual is a practical quick-reference guide to the diagnosis and treatment of renal disorders. The book covers all common renal problems in a user-friendly outline format designed for rapid information retrieval. Coverage includes acute and chronic kidney diseases, fluid and electrolyte disorders, acid-base disturbances, urinary tract infections, kidney stones, and hypertension.
Highlights of this Seventh Edition include updated information on kidney disease in diabetes. A chapter on drug dosing in patients with renal impairment provides specific recommendations for over 500 drugs.
Subcortical spongy changes of the white matter. The cortex above is spared. The dark stained neurons are not affected.
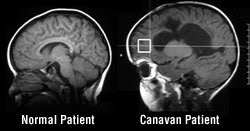
Canavan disease, one of the most common cerebral degenerative diseases of infancy, is a gene-linked, neurological birth disorder in which the white matter of the brain degenerates into spongy tissue riddled with microscopic fluid-filled spaces.
It occurs due to a deficiency of the enzyme called Aspartoacylase, since the gene which usually tells the body to produce this enzyme is faulty. Babies are born apparently unaffected. At 2 to 4 months of age, he/she develops poor head control and seizures.
Renal Failure from Vitamin C after Transplantation
A 31-year-old woman with bilateral nephrectomy due to bleeding angiomyolipomas from tuberous sclerosis received a kidney transplant with good early graft function. Irreversible, oliguric renal allograft failure soon developed from widespread deposition of calcium oxalate crystals, involving 30% of tubules (Panels A and B, hematoxylin and eosin). The patient ..........
A 76-year-old male nursing home resident with dementia and end-stage renal disease who was undergoing hemodialysis was admitted to the hospital after a syncopal episode that occurred during dialysis. Torsades de pointes was noted on telemetry monitoring.
When a urinary catheter was placed, purple urine was drained. The patient had no fever, lower urinary tract symptoms, or leukocytosis.
The urinalysis showed a pH of 9.0 and bacteriuria but no hematuria or pyuria. The urine culture showed 10 power 5 colony-forming units or more per milliliter for both Pseudomonas aeruginosa and enterococcus species. Over the next 3 days, the urine gradually became yellow and clear, in the absence of antibiotic treatment.
Purple discoloration can occur in alkaline urine as a result of the degradation of indoxyl sulfate (indican), a metabolite of dietary tryptophan, into indigo (which is blue) and indirubin (which is red) by bacteria such as Providencia stuartii, Klebsiella pneumoniae, P. aeruginosa, Escherichia coli, and enterococcus species. The clinical course is benign, and the urine typically clears with resolution of the bacteriuria and acidification of the urine. This patient had no further episodes of torsades de pointes and returned to the nursing home in stable condition.
Renal infarction due to acute renal artery occlusion. (A)An initial nephrotomogram demonstrates a thin cortical rim surrounding the right kidney (arrows), reflecting viable renal cortex perfused by perforating collateral vessels from the renal capsule. (B) Four months later, a repeat nephrotomogram shows a marked decrease in the size of the atrophic right kidney (arrowheads).
Imaging Findings : Global shrinkage of the kidney with absent opacification. There may be a peripheral rim of opacified cortex during the nephrogram phase (probably reflects viable renal cortex perfused by perforating collateral vessels from the renal capsule).
NOTE : Renal occlusion is most commonly secondary to an embolism from the heart. A decrease in renal size is detectable within 2 weeks and reaches its maximum extent by 5 weeks. Compensatory enlargement of the contralateral kidney (in individuals young enough to provide this reserve).
Electron microscopy shows massive expansion of the mesangium by fibrillar material with randomly oriented thin fibrils with a diameter of 10 to 12 nm, often extending to basement membranes as in this case (transmission electron microscopy; original magnification x8,000).
By electron microscopy, amyloid appears as randomly oriented thin fibrils, 10 to 12 nm in diameter, with a loose, flocculent background (transmission electron microscopy; original magnification x51,250).
Amyloid infiltration through the basement membrane with resulting feathery spikes with basement membrane material and delicate amyloid fibrils are shown in this case (transmission electron microscopy; original magnification x20,250).
The ProGuide™ Chronic Dialysis Catheter features a unique apposition deflection feature (the "bump") designed to minimize recirculation and optimize flow rates even when positioned against the vessel wall. ProGuide™ is the first in a series of innovative dialysis products designed for the needs of interventionalists.
Renal infarction due to acute renal artery occlusion. (A)An initial nephrotomogram demonstrates a thin cortical rim surrounding the right kidney (arrows), reflecting viable renal cortex perfused by perforating collateral vessels from the renal capsule. (B) Four months later, a repeat nephrotomogram shows a marked decrease in the size of the atrophic right kidney (arrowheads).
Imaging Findings : Global shrinkage of the kidney with absent opacification. There may be a peripheral rim of opacified cortex during the nephrogram phase (probably reflects viable renal cortex perfused by perforating collateral vessels from the renal capsule).
NOTE : Renal occlusion is most commonly secondary to an embolism from the heart. A decrease in renal size is detectable within 2 weeks and reaches its maximum extent by 5 weeks. Compensatory enlargement of the contralateral kidney (in individuals young enough to provide this reserve).
A 70 year old diabetic has chronically deteriorating renal function. An intravenous urogram reveals ring shadows and filling defects within dilated calyces. The most likely diagnosis is
a) pelvi-ureteric obstruction
b) horse-shoe kidney
c) medullary sponge kidney
d) renal tuberculosis
e) renal papillary necrosis
The correct answer is ( E )
Explanation Clinically, renal papillary necrosis is a spectrum of disease, most common in patients with diabetes, analgesic nephropathy or sickle cell disease. Patients may have an acute fulminating illness with rapid progression or may have a chronic disease that is incidentally discovered on excretory urography. Some patients may chronically pass necrotic tissue in their urine , and some may never pass papillae.
Although the diagnosis may be made from the passage of necrotic papillae in the urine, most often it is made from the excretory urogram. The radiographs show various degrees of renal involvement with either medullary or papillary changes causing irregular sinuses or medullary cavities or classic ring shadows. Retained necrotic papillae may calcify, especially in association with infection. Furthermore, this necrotic tissue may form the nidus for chronic infection. Opportunistic fungal infections have been reported. Renal sonography may be useful to diagnose papillary necrosis.
A 70 year old diabetic has chronically deteriorating renal function. An intravenous urogram reveals ring shadows and filling defects within dilated calyces. The most likely diagnosis is
a) pelvi-ureteric obstruction
b) horse-shoe kidney
c) medullary sponge kidney
d) renal tuberculosis
e) renal papillary necrosis
The correct answer is (E)
Explanation Clinically, renal papillary necrosis is a spectrum of disease, most common in patients with diabetes, analgesic nephropathy or sickle cell disease. Patients may have an acute fulminating illness with rapid progression or may have a chronic disease that is incidentally discovered on excretory urography. Some patients may chronically pass necrotic tissue in their urine , and some may never pass papillae. Although the diagnosis may be made from the passage of necrotic papillae in the urine, most often it is made from the excretory urogram. The radiographs show various degrees of renal involvement with either medullary or papillary changes causing irregular sinuses or medullary cavities or classic ring shadows. Retained necrotic papillae may calcify, especially in association with infection. Furthermore, this necrotic tissue may form the nidus for chronic infection. Opportunistic fungal infections have been reported. Renal sonography may be useful to diagnose papillary necrosis.
A 55-year-old man presents with a history of hypertension that is becoming more diffi cult to control despite the use of three antihypertensive drugs over the last two years. Clinical examination reveals a vascular bruit in the region of the right kidney. Renal function is normal. An MR angiogram of the renal arteries was performed..
Right Answer :Renal artery stenosis- The right kidney is signifi cantly smaller than the left. - There is ostial stenosis of the right renal artery.